
No matter what kind of neurovascular challenge you face, we are prepared to support you with state-of-the art screening technologies, advanced therapies and the latest endovascular options. These conditions can develop over time or come without warning, and sometimes can be life-threatening emergencies. Whether you have an aneurysm or a rare blood-vessel disorder, we as endovascular Interventional specialists can provide the care you need.
A stroke occurs when the blood supply to part of your brain is interrupted or reduced, preventing brain tissue from getting oxygen and nutrients. Brain cells begin to die in minutes.
A stroke is a medical emergency, and prompt treatment is crucial. Early action can reduce brain damage and other complications.
The good news is that many fewer Indians die of stroke now than in the past. Effective treatments can also help prevent disability from stroke.
Many factors can increase your stroke risk. Potentially treatable stroke risk factors include:
If you or someone you're with may be having a stroke, pay particular attention to the time the symptoms began. Some treatment options are most effective when given soon after a stroke begins.
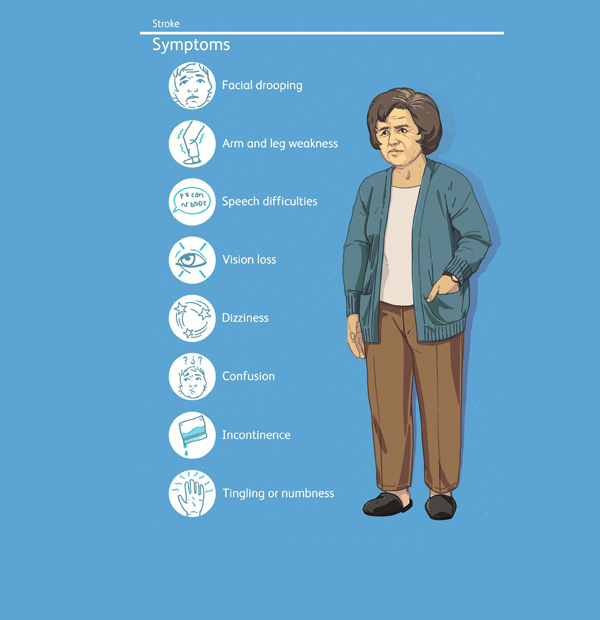
Signs and symptoms of stroke include:
A stroke can sometimes cause temporary or permanent disabilities, depending on how long the brain lacks blood flow and which part was affected. Complications may include:
Seek immediate medical attention if you notice any signs or symptoms of a stroke, even if they seem to come and go or they disappear completely. Think 'FAST' and do the following:
The treatment for ischemic stroke is clot removal. Vascular and Interventional Radiologist can accomplish this with medication and mechanical treatments:
An endovascular procedure or a mechanical thrombectomy is a strongly recommended option to remove a clot in eligible patients with a large vessel occlusion or LVO.
The procedure:
We have very fast and competent working team which provide you comfortable atmosphere and ease your nerves. Usual time of stay is around 2-3 Days.
Resume to work?
You can resume your work after 1 week if existing disease allows.
The carotid artery is in the neck. There are usually two carotid arteries, one on each side of the neck The brain is supplied with blood from the two carotid arteries, along with two other arteries (the vertebral arteries), joining together to ensure the brain receives the blood that it needs.
Carotid artery disease causes strokes and carotid artery treatment is intended to reduce the risk of strokes in the future. The source of the blood clots may be the carotid artery causing stroke these clots get carried to the brain, and cause blockage of is artery, and the loss of blood to the area of the brain supplied by the artery. This may lead to permanent loss of brain function (this area dies). The greater the narrowing in the carotid artery, the more likely it is that this will cause clot, both now and in the future. For this reason, if symptoms occur, Stroke like, a doctor may recommend that this be treated. Sometimes the narrowing in the carotid may be very severe, but still not cause symptoms. In such circumstances, despite the fact that the narrow area has not caused problems, a doctor may advise that this be treated to try to prevent strokes. On the other hand, some blood clots can form in carotid arteries where the degree of narrowing is relatively slight. In this situation, treatment with drugs is usually recommended.
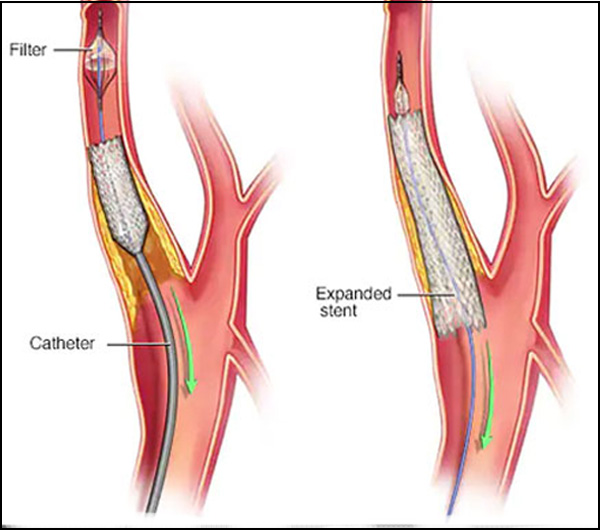
There are a number of stents that have been specially designed to be placed in the carotid artery. These have been designed specifically for the needs of this artery at the place where the artery divides. If disease should occur lower down in the carotid artery, then stents often used in other areas are suitable.
The specific stents made for the carotid artery are all “self expanding”. What this means is that they are made of metal, which springs open to a predefined size. The stents are pressed down onto their delivery system , where they are kept very thin to allow them to be passed to where they are needed. They are then released, in a controlled fashion, so that they fill the artery, and push the unwanted material out of the way. Often it is necessary to help the stent to open to the correct size, by finally expanding them with a balloon.
If there is disease either in the chest or up close to the brain, “balloon mounted” stents are often used. These will not expand to size on their own, so they are put onto the balloons and expanded up to size once this has been put into the correct place. The balloon is then deflated, leaving the stent in place. These stents have the advantage of being easier to place in the correct position, but the disadvantage of not being able to withstand compression. If these stents are compressed, they lose their shape and may cause the artery to block. They are, therefore, not suitable for use in the neck, where they may be compressed by outside forces and movement, where the self expanding stents are used.
Complications from carotid artery stenting can be considered either as occurring around the time of the procedure (within 30 days of the procedure) or later. The list below is not exhaustive, but rather is intended to explain the more common or worrying problems that may occur.
As indicated in the section on the complications of carotid artery stenting, stroke can occur at the time of the procedure, and subsequently. A number of steps can be taken by the medical team to reduce the risk:
The procedure:
All people who are known to have carotid artery disease will have their medications altered to try to reduce their risk of stroke or further stroke.
When the level of carotid artery disease goes above a critical level additional treatment is often recommended. This can be in the form of either an operation (carotid endarterectomy – see VS SITE) or carotid artery stenting. carotid artery stenting offer the potential benefit of preventing stokes in the future.
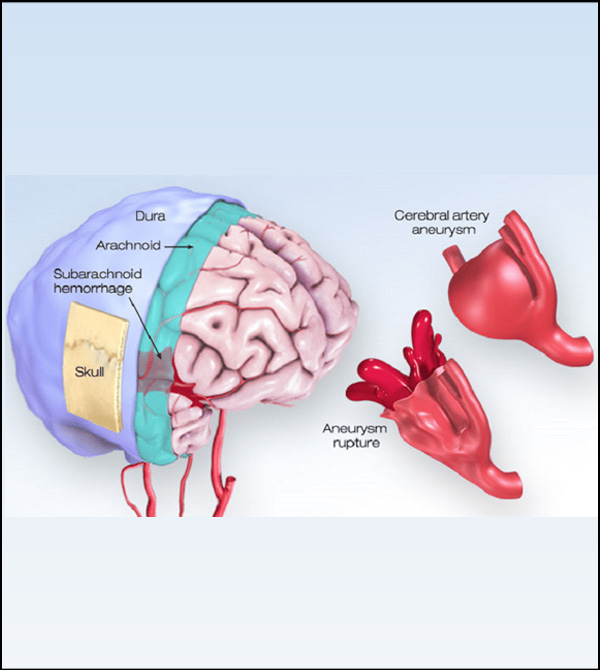
An aneurysm is an abnormal outpouching of an artery's wall. Aneurysms affecting the arteries supplying the brain can cause a stroke. If the aneurysm ruptures, blood flows into the space surrounding the brain called the subarachnoid space. A patient with a subarachnoid hemorrhage usually suffers a severe headache followed by nausea, vomiting, irritation and lethargy. Double vision, neck stiffness, weakness, loss of sensation, and loss of consciousness can also occur.
Brain aneurysms are more common in adults than in children and more common in women than in men.
Some of these risk factors develop over time; others are present at birth.
If left untreated an aneurysm may rupture leading to life threatening bleeding and somtimes death
Seek immediate medical attention if you develop a:
Sudden, extremely severe headache
To diagnose a brain Aneurysms, your neurologist or Interventional Radiologist will review your symptoms and conduct a physical examination.
Your doctor may order one or more tests to diagnose your condition. Interventional Radiologists trained in brain and nervous system imaging usually conduct imaging tests.
Tests used to diagnose brain Aeurysms include:
There are two basic approaches to treating an aneurysm:
With this approach, small platinum coils are placed into the bulge of the aneurysm to seal it off while preserving the normal blood flow of the artery.
This procedure does not require a craniotomy or any incision on the head. The procedure is done in a radiology suite where angiograms are done. It is done under general anesthesia.
During the procedure, a small tube is placed through an artery in the groin. Small platinum coils are delivered to the aneurysm . They block off the ballooned part of the artery. The normal opening of the artery is left clear
We have very fast and competent working team which provide you comfortable atmosphere and ease your nerves. Usual time of stay is around 2-3 Days.
Resume to work?
You can resume your work very next day of the procedure preferably in 2- 3 days.
Copyright © 2024 All Rights Reserved by Dr. Ashutosh Kharche

