Interventional radiology has become an integral part of patient care services offered at many secondary and tertiary care hospitals in India. In addition to the routine elective consultation and procedural care for various vascular, nonvascular, and oncologic conditions, the interventional radiology service is being increasingly involved in the treatment of emergency conditions such as acute stroke or acute pulmonary embolism, deep venous thrombosis, Acute arterial thrombosis, Acute Bleeder managements. The emergency interventional radiology service is more challenging compared with the elective service in several aspects, including, but not limited to, the need for quick decision-making given the clinical status of the patient, availability of resources for early intervention, and availability of alternative therapeutic options. As interventional radiologists, we are committed to providing emergency interventional services. It is important that we, as a society, work together with the hospitals in laying guidelines for emergency interventional radiology service. This would not only improve the patient care and visibility of interventional radiology as one of the pillars of medicine but also enhance the appeal of interventional radiology as a specialty for future medical graduates
Veins are the blood vessels that transport blood from various body parts to the heart.
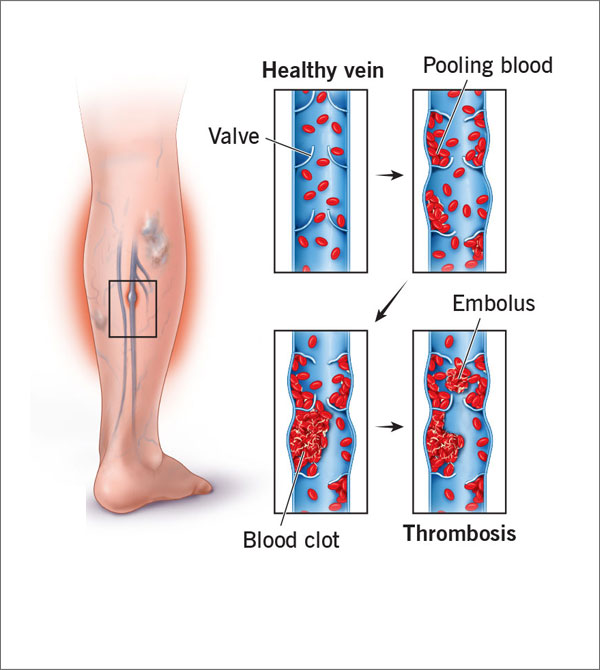
A serious medical condition in which a blood clot is formed in a vein deeply inside body is called Deep vein thrombosis (DVT). A blood clot that mostly is in a jelly like state is formed in the veins. It is normally observed that DVT occurs in the thigh or lower leg area, however Deep Vein Thrombosis can happen in any other areas of human body.
Sometimes condition of Deep Vein Thrombosis is also sometimes referred as Post Thrombotic Syndrome, Post Phlebitic Syndrome & Thromboembolism though the former two are conditions which are outcome of prolonged existence of DVT.
Sometimes the clot so identified as DVT breaks free, and flow to other vital organs in the body. Incidence wherein clots are observed to block flow to lungs is called pulmonary embolism and is considered life threatening.
There is no single factor identified to be the cause of DVT. DVT as condition is observed to be developed due to various factors or combination thereof. Some of the factors which are known to be the cause of DVT or which increase the probability of a person developing Deep vein Thrombosis are listed below:
DVT is difficult medical condition to identify as many patients (50%) may not display any symptoms. Also, the symptoms are more generic and are shared among various medical conditions. Patients may not be aware of DVT till they experience a serious life-threatening medical incidence like pulmonary embolism. Some of the common symptoms are:
While the above symptoms may appear generic and one may not feel the need of medical evaluation, it is to be remembered that DVT leads to lethal incidences like Pulmonary Embolism hence shouldn’t be ignored.Patients experiencing above symptoms are advised for medical treatment, below are listed some symptoms which a patient having life-threatening incidence of Pulmonary Embolism may experience and hence should be immediately evaluated by qualified medical professionals.
Primary evaluation of DVT is done by conducting a physical evaluation by medical professional. Clinical confirmation of DVT is done by performing some of the below mentioned tests as required by the medical doctor.
Post-thrombectomy evaluation of the venous segment may reveal areas of venous compression, stenosis or recalcitrant thrombus in some of the patients. May-Thurner anatomy is the most common anatomic variant found on completion imaging during the treatment of proximal DVT . This syndrome is characterized by compression of the left common iliac vein by the right common iliac artery against the fifth lumbar vertebra, resulting in venous compression, development of venous scar tissue and eventually venous stenosis. This condition then predisposes the patient to left iliofemoral DVT. With anticoagulation alone, untreated iliac vein obstruction prevents vessel recanalization in 70–80% of patients and clot propagation may continue in up to 40% of cases. Further, patients with iliofemoral DVT and untreated May-Thurner anatomy experience an increased risk of recurrent DVT and universally experience symptoms of post-thrombotic syndrome during follow-up. Adequate treatment of anatomic compression, stenosis or persistent small thrombus after CDT or PMT requires angioplasty and stenting.
While nothing much can be done to change the heredity, risk of developing Deep Vein Thrombosis can be greatly reduced by adopting a healthy and active lifestyle.
Patients are anticoagulated post procedure with unfractionated heparin or low-molecular-weight heparin and transitioned to oral warfarin/ Newer anticoagulatns for 6 months (goal international normalized ratio 2.0–3.0). Patients with recurrent DVT or hypercoagulable disorders may require a longer duration of anticoagulation and consultation with primary care physicians is recommended. Patients with venous stents require lifelong aspirin therapy. Follow-up with duplex ultrasonography is also recommended at 1- and 6-month intervals and yearly thereafter.
We have very fast and competent working team which provide you comfortable atmosphere and ease your nerves. Usual time of stay is around 2-3 Days.
Resume to work?
You can resume your work very next day of the procedure preferably in 2- 3 days.
Copyright © 2024 All Rights Reserved by Dr. Ashutosh Kharche

