Children and adults with vascular malformations are best managed with a multidisciplinary team of specialists. Interventional radiology may deliver primary treatment such as staged sclerotherapy and embolization for malformations that are poor candidates for primary surgical resection or play a supportive role such as preoperative or intraoperative embolization. A thorough understanding of vascular morphology and flow dynamics is imperative to choosing the best treatment tool and technique.
Our minimally invasive image-guided treatments effectively treat patients with minimal discomfort.Children and adults with vascular malformations are best managed with a multidisciplinary team of specialists. Interventional radiology may deliver primary treatment such as staged sclerotherapy and embolization for malformations that are poor candidates for primary surgical resection or play a supportive role such as preoperative or intraoperative embolization. A thorough understanding of vascular morphology and flow dynamics is imperative to choosing the best treatment tool and technique.
A vascular malformation is an abnormal development of blood vessels. They might be found in the large arteries and veins, in smaller vessels called arterioles and venules, in microscopic capillaries, and/or in the lymphatic channels that carry lymphatic fluid and white blood cells outside of the arteries and veins.
Vascular malformations are most easily categorized based on the type(s) of vessels involved and how blood flows through them. They include the following:
Slow-flow vascular malformations include venous and lymphatic malformations.
Venous malformations:
These are the most common vascular malformations. They affect the veins, which carry blood from organs back into the heart and lungs for re-oxygenation. They can occur anywhere in the body, and they can be isolated or part of a syndrome, most commonly Klippel-Trenaunay Syndrome.These venous malformations tend to be identified later in life; typically, symptoms are triggered by an injury, or physiological changes such as puberty or pregnancy. Sometimes they are found incidentally, during MRI studies for other conditions. Symptoms suggesting a possible venous malformation range from minor aches and pains to recurrent bouts of bleeding, clotting disorders and organ damage, mostly within bones, joints and skeletal muscles.
Lymphatic Malformations:
The lymphatic vessels carry lymphatic fluid and white blood cells outside of the arteries and veins. Malformations affecting the lymphatic channels may start to cause problems during infancy and early childhood. They can cause pooling of the lymph fluid into cysts or fluid-filled pockets of various sizes. These cysts, in turn, can develop problems such as infection, bleeding and erosion into adjacent organs.
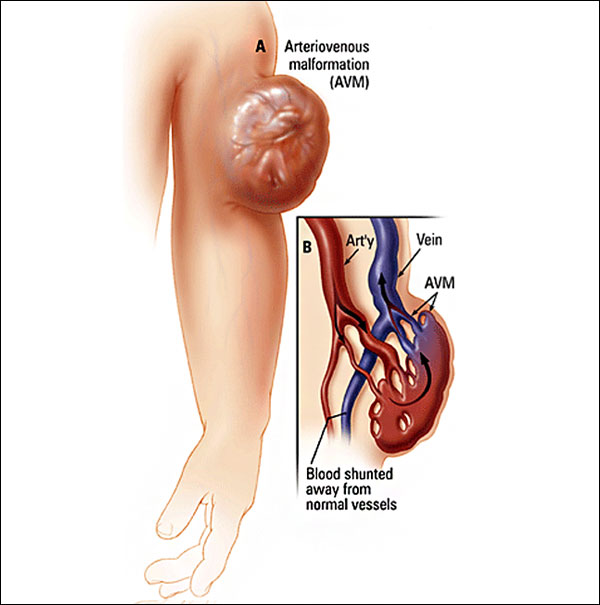
Fast-flow arteriovenous malformations develop as the result of an abnormal connection between arteries that supply the body’s organs, and the veins, which drain them. Picture these as being like short-circuits: Blood pumped from the heart to a given organ can’t get there and is instead sent back toward the heart. The draining veins become dilated and engorged, the target organ is deprived of needed oxygen and nutrients, and–in the worst scenarios—heart and/or organ failure can develop
Arteriovenous malformations can occur anywhere in the body, but are most typically found in the brain, spinal cord and extremities. It is rare, but possible, for arteriovenous malformations to be found in the internal organs, including the kidneys, the intestines and the lungs. While there is currently no cure for arteriovenous malformations, various treatment options exist aimed at slowing their growth, and minimizing and at times eliminating symptoms.
There are several congenital mixed syndromes that involve vascular malformations.
Your doctor will have a suspicion or a good indication that you have an AVM on the basis of the history you provide and on physical examination or in some circumstance your family history. Your doctor will refer you to a Endovascular Interventional Radiologist who are recommended specialist.
The diagnosis is typically clinical and imaging the lesion is key to understand the size and nature of the lesion. Imaging can also help decide when and how to treat these lesions. Ideally AVMs should be managed by a ‘multi-disciplinary’ team of doctors, nurses and specialists with a specific interest and experience in diagnosing and treating this condition.
AVMs are very complicated. It is important that treatment and follow up is carried out and supervised by an endovascular interventional Radiologist team.
Treatment options range from endovascular therapy to Surgery to Endovascular therapy.
This is defined as the intentional occlusion of the blood vessels that make up the AVM. This is carried out in conjunction with an angiogram (see earlier). Depending on the embolisation agent and access technique used by the Interventional Radiologists a general anaesthetic may be required.
Embolisation of these lesions typically involves one of two techniques:
Treatment options are divided up in to conservative management, percutaneous injections (Sclerotherapy) or surgery or a combination of these. If there are no symptoms then there is no indication or need for treatment.
Initially it important to determine the exact symptoms and to what degree this is distressing the patient and how much of an impact this is having on their life. The majority of venous malformations do not need treatment, but this can be reviewed at any time, especially if symptoms worsen or change. Venous malformations are not malignant and do not have malignant potential.
Conservative management includes pain relief with anti-inflammatory tablets, compression dressings if the lesion is in a limb and alteration of lifestyle accordingly. This approach is usually advised if symptoms are well tolerated.
Treatment depends on the number of vascular spaces within the lesion and the amount of more solid tissue. Lesions with a more spacious component (ie: more venous lakes) are more suitable for injection therapy or ‘sclerotherapy’ than those that are predominantly solid in nature. Depending on the site, size amongst other factors certain lesions are suitable for surgical removal.
Sclerotherapy is a type of treatment that involves the injection of a special chemical into the venous malformation to ultimately shrink it and relieve the symptoms it is causing. Various substances can be used but most commonly the chemical used is Sodium Tetradecyl sulphate (Fibrovein). When injected into a lesion it causes an inflammatory reaction which leads to localised blood clots and the formation of a scar in place of the venous malformation. This corresponds to shrinkage of the malformation. This is carried out under ultrasound and x-ray control as the doctor needs to be sure that the correct part of the malformation is accessed with the needle and needs to assess the degree of communication with adjacent communicating veins.
Often a ‘course’ of multiple injections are required to adequately treat a venous malformation and it can be some time before the patient notices a significant difference. Not all venous malformations are successfully treated in this way but in the vast majority of cases significant results are achieved.
It is typically carried out as a day case procedure in hospital.
Immediately after the injection considerable swelling can occur along with pain. This usually settles within days – weeks of the injection. Pain is usually adequately treated with oral pain killers. It is when this swelling settles that there is a noticeable reduction in the size and / or symptoms of the malformation.
There is a small risk of infection and bleeding but as sclerotherapy is carried out via a needle puncture and not an incision this is unusual.
Bleomycin is widely used as a chemotherapy agent to treat certain types of cancer. Vascular anomalies are not cancers but bleomycin has been shown to be effective in treating certain types of vascular anomalies when injected directly into the lesion, rather than into the bloodstream as with chemotherapy. Subtypes of vascular anomalies successfully treated include, lymphatic malformations (macro and microcystic) and even venous malformations. Bleomycin works by exerting its effect on the lining of the malformation and preventing further growth and promoting regression. It does this by inhibiting local DNA synthesis. Results are encouraging with its use. This form of treatment often requires a course of injections over a period of months. Bleomycin treatment is considered in a multi-disciplinary setting following discussion with the patient and review of cross-sectional imaging. It can be considered as a first line treatment in micro-cystic lymphatic disease.
Very small risk of bleeding and bruising at the puncture site and infection along with a small risk of damaging the blood vessels as the catheter is advanced.
Pain is often encountered following the procedure but this is usually short-lived and may last a few days.
Swelling is sometimes experienced at the site of treatment and is related to the local inflammatory process caused by blocking the blood vessels and sometimes by the embolic agent itself.
The risks will be discussed with you prior to any procedure but are generally low as embolisation is proven as a safe and effective method of treating AVMs worldwide
We have very fast and competent working team which provide you comfortable atmosphere and ease your nerves. Usual time is day care.
Resume to work?
You can resume your work very next day of the procedure preferably in 2- 3 days.
Copyright © 2024 All Rights Reserved by Dr. Ashutosh Kharche

