Autogenous arteriovenous fistulas (AVF) and prosthetic arteriovenous grafts (AVG) are necessary for chronic end-stage renal failure patients on hemodialysis. AVFs are the preferred initial hemodialysis access due to their longer patency than AVGs. AVGs, however, remain clinically important in patients whom AVFs are not feasible, and possibly in special populations such as the elderly.Hemodialysis accesses are prone to failure due to thrombosis, usually concomitant with stenosis over the anastomosis or outflow vein. Access thrombosis frequently requires semi-emergent salvage intervention, but outcomes are generally unfavorable. Patients eventually may require multiple salvage procedures to restore functionality or creation of a new access. Some patients require placement of central venous catheters in the interim whilst the hemodialysis access becomes fully functional. Alternatively, to prevent access failure, clinicians can monitor the performance of these accesses and prophylactically provide interventions to rectify the hemodynamic problems and prolong their patency. Our service currently provides endovascular interventions to haemodialysis patients with failing access.
Dialysis allows people with kidney failure (renal failure) a chance to live productive lives. When kidney function decreases to a critical level or complications arise, a person may need to start dialysis. There are two main types of dialysis, hemodialysis and peritoneal dialysis.
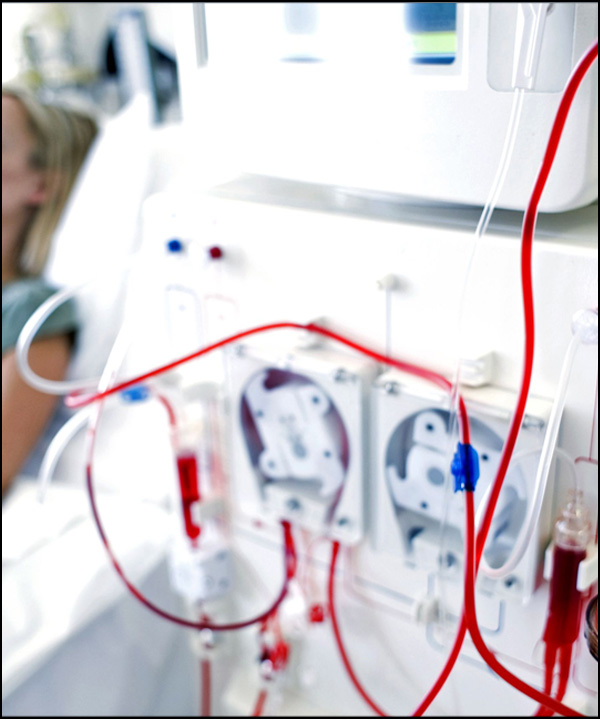
Hemodialysis is a procedure that withdraws blood from the body into a machine that uses a special membrane (dialyzer) to filter wastes and remove extra fluid from the blood. Hemodialysis also restores the electrolyte balance in the blood.
Because of the need to remove blood from the body and replace it during hemodialysis, a means for accessing the patient's blood circulation -- called 'vascular access' -- is necessary. There are three different techniques for this, some of which are used interchangeably: Catheter- Temporary or Permanent (Permacath), Dialysis fistula, Graft. All of these techniques are able to withdraw and replace large amounts of blood at the same time - about one quart per minute.
The most desirable form of hemodialysis vascular access is called a fistula. To make a fistula, a surgeon connects an artery to a vein in the forearm or upper arm. With time, usually one to three months, the vein enlarges and becomes ready to receive the needles used to withdraw and replace blood during dialysis. A fistula can last for many years if the vein enlarges and the fistula 'develops'. About three-quarters of fistulas develop or mature. During the time that a fistula is developing, if hemodialysis is necessary, another form of vascular access will be necessary, usually a catheter.
In some patients, the arteries and/or veins are not suitable for making a fistula. In these patients, a shunt (or graft) can be used as an alternative form of dialysis access. A graft is a piece of plastic tubing that is inserted by a surgeon and connects the artery to the vein. Unlike fistulas, grafts do not need to 'develop' and are ready for use in most instances by four weeks after placement. A catheter may be necessary for dialysis during this waiting period. The disadvantage of grafts is that they do not last nearly as long as fistulas and can develop narrowing and clotting more frequently. In addition, grafts can get infected -- something which does not happen very often with fistulas. Just as with fistulas, narrowing veins with grafts can be detected before they clot if the appropriate screening techniques are used. These include self-examination, measuring flows during dialysis with a special machine, and checkups by an interventional radiologist. Once an abnormality is detected, you need to be scheduled to have it treated by Interventional Radiology as quickly as possible. It is very important that patients keep their appointments with Interventional Radiology so that clotting does not occur. If clotting does occur it can be treated by an interventional radiologist.
We offer the following ways to establish and maintain your dialysis access.


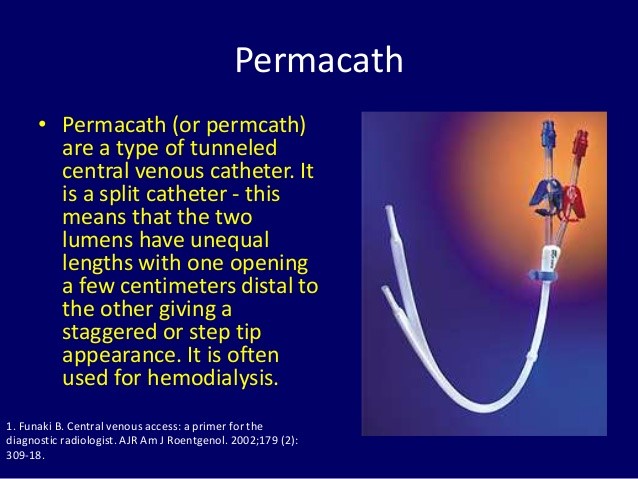
A permacath is a piece of plastic tubing that is similar to a jugular catheter. It is used for hemodialysis in the exact same way that a jugular catheter is used. The advantage of the permacath is that it can provide access to the
vascular system for up to one year. This is important for dialysis patients because they will avoid multiple catheter insertions, which could eventually lead to vein damage.
PERMCATH procedure
Using an X-Ray machine and small surgical tools, the surgeon places the permacath in the jugular vein. The permacath is moved under the skin throughout the upper chest, under the collarbone, and the end of the catheter comes out on the chest wall. The X-Ray is used in order for the surgeon to follow the path of the catheter throughout the procedure and make sure it is placed correctly.Risks include puncturing the lung, bleeding, and infection.
While a fistula is considered the best kind of access, problems can occur, including vein narrowing, or stenosis and clotting, or thrombosis. We as Vascular and Interventional radiologist offer the following ways to establish and maintain your dialysis access.
Benefits:
Some blockages of the veins or arteries are too difficult to open with catheters and balloons. Surgery may be needed to bypass the blockage. If that is the case, a dialysis catheter may need to be placed in a neck vein to allow you to receive dialysis temporarily until a surgeon is able to fix or revise your dialysis fistula or graft.
We have very fast and competent working team which provide you comfortable atmosphere and ease your nerves. Usual time of stay is around 2-3 Days.
You can resume your work after 2-3 days if existing disease allows.
Copyright © 2024 All Rights Reserved by Dr. Ashutosh Kharche

