An aortic aneurysm is an abnormal bulge that occurs in the wall of the major blood vessel (aorta) that carries blood from your heart to your body. Aortic aneurysms can occur anywhere in your aorta and may be tube-shaped (fusiform) or round (saccular).
Aortic aneurysms include:
In some cases, an individual may have an abdominal aortic aneurysm and a thoracic aortic aneurysm.
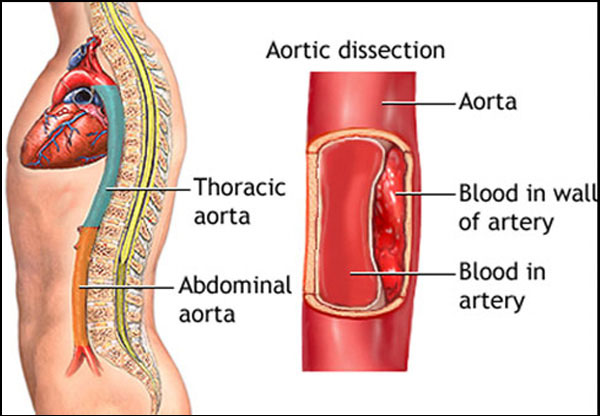
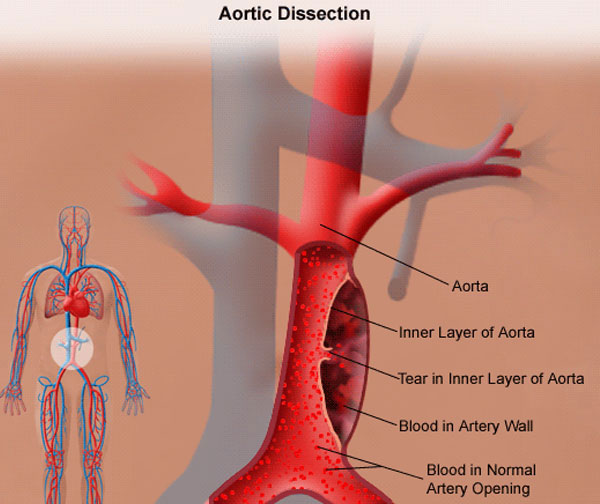
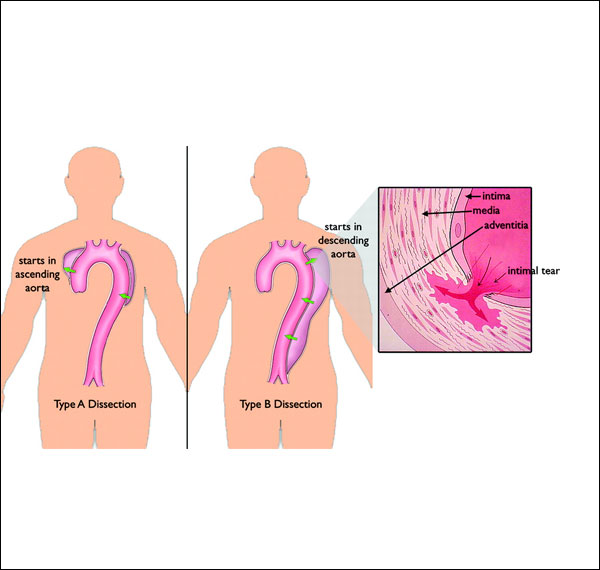
Having an aortic aneurysm increases your risk of developing an aortic dissection or rupture leading to death
We offer the best treatment of Aortic repair i.e Endovascular aneurysm repair which involves inserting a graft within the aneurysm through small groin incisions instead of an Open Surgery using X-rays to guide the graft into place.
The advantage of this type of repair is that there is no abdominal surgery. This technique is therefore safer than the traditional operation, and you need to spend less time in hospital. A disadvantage is that some patients have to undergo a further operation at a later stage to refine the initial procedure.
The aorta is the main artery from the heart and carries blood to the organs and limbs. An aortic aneurysm is an enlargement of the aorta. In the abdominal aorta an aneurysm is defined as an enlargement of the aorta of at least 1.5 times its normal diameter, or greater than 3 cm diameter in total.
Most are caused be atherosclerosis ('furring/hardening of the arteries'). Rarely the artery wall is weakend by hereditary conditions main risk factors for AAA include smoking, high blood pressure, increasing age and a family history of aneurysms.
Most aneurysms do not produce any symptoms.
Occasionally they can cause abdominal or back pain, or even a pulsating sensation in the abdomen. However, pain in a patient with a known aneurysm can be a sign of impending rupture and urgent medical attention should be sought.
Most aneurysms are found incidentally (by chance) when tests are carried out for other reasons or are picked up by screening.
The most serious risk is that the aneurysmal blood vessel can eventually enlarge until it bursts. This bleeding is usually life threatening and urgent surgery is needed. 80% of patients with a ruptured AAA will not survive. Unfortunately, even with emergency surgery, only about half survive beyond 30 days. Rupture can be avoided if the aneurysm is repaired before this occurs.
The risk of rupture increases with the size of the aneurysm. An aneurysm of 6 cm in diameter has an annual risk of rupture of 25%. Symptoms of rupture can include; Sudden severe abdominal or back pain. This may be accompanied by signs of shock (collapse, light headedness/dizziness, rapid heart beat, fainting, nausea and vomiting, excessive thirst, sweating). Immediate medical attention must be sought.
If there is a high risk of an aneurysm/dissection or you have been detected to have one, you could consult an Interventional Radiologist .
A detailed physical examination and blood investigation should be done for assessing the fitness of the patient for treatment. If there is no contraindication a computed tomography angiography (64 slice minimum) should be performed. A CT scan will give the location, exact dimensions and relationship of the aneurysm to the main branch arteries of the body. This will help plan whether treatment is required and what sort of treatment should be planned. In few cases if a CT scan cannot be performed or if additional information is required, then a digital subtraction angiogram (DSA) or a magnetic resonance imaging (MRI) may be done. Size is an important criterion for aneurysms. The normal aorta in the chest measures 2.5-3.2 cms, and in the abdominal aorta measures 1.8-2.3 cms. If the thoracic or abdominal aneurysm is less than 4.5 cms in its maximum diameter, then medical management is advised with regular radiologic follow up. If the size is greater than 4.5cms then treatment should be planned. In cases of dissections, detailed discussion and planning has to be done to decide the treatment, which are now successfully treated by the endovascular method.
Your doctor may recommend surveillance (watch and wait) or Surgical Repair. The decision will depend on the size and type of aneurysm, the short and long term benefits/risks of surgical repair; and your physical fitness. The main surgical options are:
1. Endovascular repair
2. Conventional open surgery
We have very fast and competent working team which provide you comfortable atmosphere and ease your nerves. Usual time of stay is around 2-3 Days.Resume to work?
You can resume your work very next day of the procedure preferably in 2- 3 days.
Copyright © 2024 All Rights Reserved by Dr. Ashutosh Kharche

